Introduction
In January 2020, the World Health Organization (WHO) declared that the global outbreak of the novel coronavirus disease known as COVID-19 constituted a public health emergency of international concern (PHEIC). A Statement on COVID-19 issued at an Extraordinary G20 Leaders’ Summit held virtually in March of the same year reaffirmed the need for quick action through international cooperation. In response, the WHO and a group of partners, initially including international organizations active in the health field, the European Union (EU), France, and private foundations, launched the Access to COVID-19 Tools Accelerator (ACTA) on April 24, 2020. The objective of ACT-A is to accelerate the development and production of COVID-19 tools and to create a framework to ensure fair and equitable access and distribution of such products. ACT-A comprises four pillars—Vaccines, Therapeutics, Diagnostics, and the Health Systems & Response Connector (HSRC, initially called the Health Systems Connector)—of which the Vaccine pillar is also known as COVAX (short for COVID19 Vaccines Global Access), with WHO acting as the global coordinator and bearing the responsibility of access and allocation.
The ACT-Accelerator Strategic Review, an ACT-A interim review report (hereafter, Strategic Review) was published in October 2021. The Strategic Review recognizes the positive achievements of ACT-A in accelerating the development, supply, and access to COVID-19 tools and recommends that, although it is a time-limited collaboration, ACT-A should continue its activities until at least the end of 2022. On the other hand, it analyzes the current situation by sorting the various challenges faced by ACT-A that have impeded the achievement of its objectives into the categories of external and internal challenges. The Strategic Review did not analyze in detail some factors identified as “external challenges” and some elements deemed outside the scope of the essential mandate of the Health Systems (& Response) Connector. I will therefore focus on these factors in this policy brief and will emphasize that in order to ensure fair and equitable access to healthcare, including access to medical tools, it is essential to have continued and consistent efforts at all levels, from grassroots to global policies, to close the gap through inclusive, democratic, and transparent decision making.
Achievements and challenges of ACT-A
(1) Disparities in access to vaccines, diagnostics, and therapeutics
Among the four pillars of ACT-A, COVAX did not function as initially hoped. This was partly because of the rise of vaccine nationalism, where high-income countries pursued bilateral contracts with vaccine manufacturers to secure priority access to vaccines and hog more than their share, leaving insufficient supply for COVAX. One thing that needs to be noted here is that the lessons learned from the 2009 influenza A H1N1 pandemic were not heeded. At the same time, an increasing number of higher-income countries have donated vaccine doses to low- and middle-income countries out of their excess domestic supply during this pandemic, but because the donations were not always well planned and various challenges arose, COVAX and its partners, AVAT and Africa CDC, were compelled to issue a joint statement calling on the international community to adhere to certain standards when donating vaccines. In terms of diagnostics as well, there are wide disparities among countries depending on their income levels. The slow pace of approval of test kits for inclusion on the WHO’s Emergency Use Listing (EUL) and insufficient technical support have been cited as key bottlenecks. It is estimated that six out of seven infected persons in Africa are undetected, and there is an urgent need to disseminate affordable rapid antigen tests that do not require sophisticated equipment. With regard to therapeutics, there is no clearly articulated joint procurement structure yet to supply countries or to negotiate contracts nor an Advance Market Commitments (AMC) mechanism for low-income countries, which puts therapeutics at risk of being hogged by higher-income countries, as was in the case of vaccines. Merck entered into a license agreement with the Medicines Patent Pool (MPP) for the manufacture of antiviral drug, Molnupiravir. It is therefore thought that most of the demand for the drug from lowerincome countries can be covered by generic drugs. However, there have been complaints that some of the upper middle-income countries experiencing severe outbreaks of COVID-19 are not covered by the MPP, and the voluntary licensing agreement between MPP and Merck includes a termination-upon-challenge clause.
(2) Perception of the health system
The Strategic Review noted that limited coordination between the WHO’s Health Emergencies Programme (WHE) and the HSC led to missed opportunities for ACT-A. Responding to this point, ACT-A announced in its Strategic Plan & Budget (October 2021 to September 2022) that the HSRC would fully integrate the WHE and UNICEF into the work of the revamped “Health Systems & Response Connector.”
Meanwhile, there were fundamental debates over the health systems pillar mandate that went beyond just the need to ensure collaboration among individual organizations. The Strategic Review notes that there was ambiguity over whether the HSC should play a humanitarian assistance role (along the lines of emergency assistance in times of disaster) or one of medium- to long-term social development, and different institutions had very different perspectives on the HSC’s goals. The Strategic Review takes the position that ACT-A’s mandate is “ending the acute phase of the pandemic,” and any work that would require a longterm perspective, such as building a stronger system to prepare for the next pandemic, is not within the mandate of ACT-A and should be carried out by a separate entity. This seems to be an extension of the idea of “equitable allocation of tools” and seems to view health systems as a means to that end. On the other hand, the Platform for ACT-A Civil Society & Community Representatives, a platform for civil society organizations (CSOs), has released statements requesting that the activities of the HSC/HSRC be centered on healthcare human resources rather than on the procurement of personal protective equipment. This request seems to take the position that mid- to long-term issues, including securing healthcare human resources, are integral to and inseparable from robust health systems as the prerequisite for the deployment of healthcare tools.
(3) Transparent and democratic governance and decision making
The Strategic Review points out that nearly two-thirds of the current member states of the Facilitation Council, a body responsible for the overall governance of ACT-A, are categorized as high-income countries, and the voices of lower-income countries may not be sufficiently represented. Also, those member states that are also members of existing governance structures of international organizations can exercise influence through other channels. Those facts and others raise the concern that decisions are sometimes made at times through processes that lack transparency, and that the voices of CSOs and community representatives (CRs) are not adequately reflected. The structure of ACT-A has been changing as new partners have joined as the collaboration proceeds. Although representatives from the pharmaceutical industry remain listed as part of the Principals Group, their corporate logos no longer appear in the organizational chart, making them less visible in the collaboration. As seen in this example, some stakeholders point out that the presentation of information is inconsistent and that accountability throughout ACT-A is unclear. While it should be appreciated that nongovernmental organizations (NGOs) and CSOs are participating to a certain extent in the governance of ACT-A and its constituent organizations, they do not necessarily have a great deal of influence, and there is some ambiguity regarding their representativeness. There is also room for improvement in terms of the gender gap in the representation of men and women in governing bodies. Who participates in decision making under what mechanisms is an important point when examining what potential bias could affect that decision making. Specific measures must be implemented to reform ACT-A from the viewpoints of promoting participation of those people who are most vulnerable to the impact of the pandemic, providing support to areas that are often neglected, and transparency of information in democratic decision making.
(4) Transmission of information and imbalances in funding
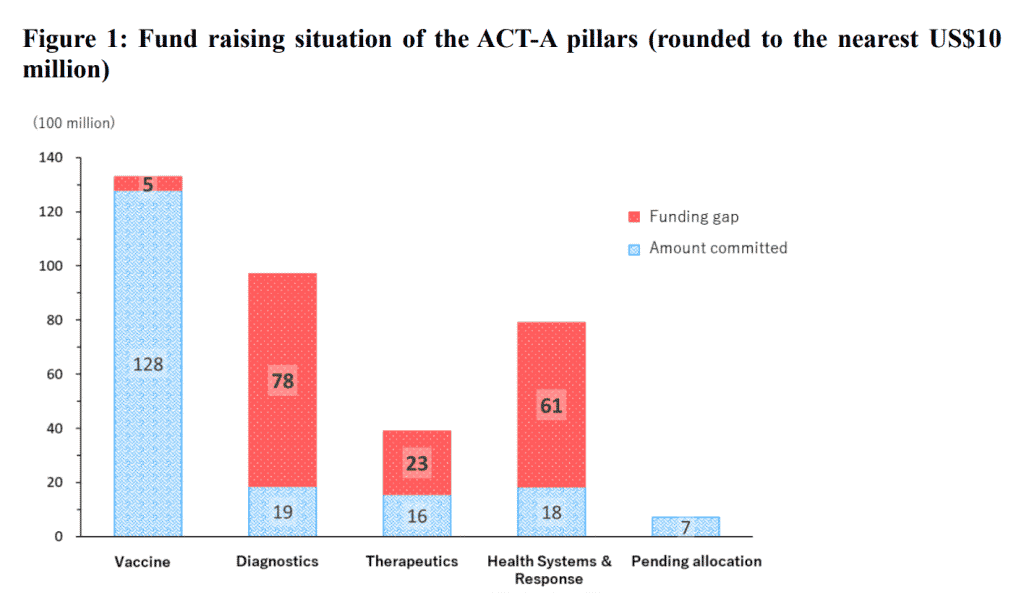
Although ACT-A does make some effort to disclose information, such as indicating its overall funding needs and publishing its progress online in a consolidated manner, there has been criticism that the full picture of ACT-A’s specific funding flows is difficult to capture. In part because of this limited visibility of the aggregate financial flows, pillars other than the vaccine pillar, which attracts the greatest attention from donors, are suffering from chronic funding shortage (fig. 1). ACT-A needs to develop a more effective communication strategy to attract adequate funding for all areas as needed. In doing so, it is important from the perspective of fair and equitable access to provide detailed and convincing explanations about those areas in which higher-income countries (who are the primary donors) are not as interested and to incorporate a grassroots-level viewpoint that incorporates the perspective of vulnerable people.